Baby Structures During Pregnancy

Fetal Structures & Ultrasound:
Prenatal Ultrasound’s role in screening baby structures.
In This Article:
-
Published
-
Last Modified
Tags

Pregnancy is a journey of discovery, not just of the self but also of the little life growing inside you. Among the many wonders this period brings is the ability to glimpse into your baby’s developing world through ultrasound screenings. Here we delve into the critical aspects of baby structures, their development, and the pivotal role of ultrasound in ensuring the well-being of your unborn child.
As expectant mothers, the health and development of our unborn child is paramount. Advances in medical technology have gifted us with the ultrasound, a window into the womb, allowing us to monitor the growth and health of our babies like never before. Understanding the structures of a developing baby provides invaluable insights into their well-being and development.
What are fetal structures?
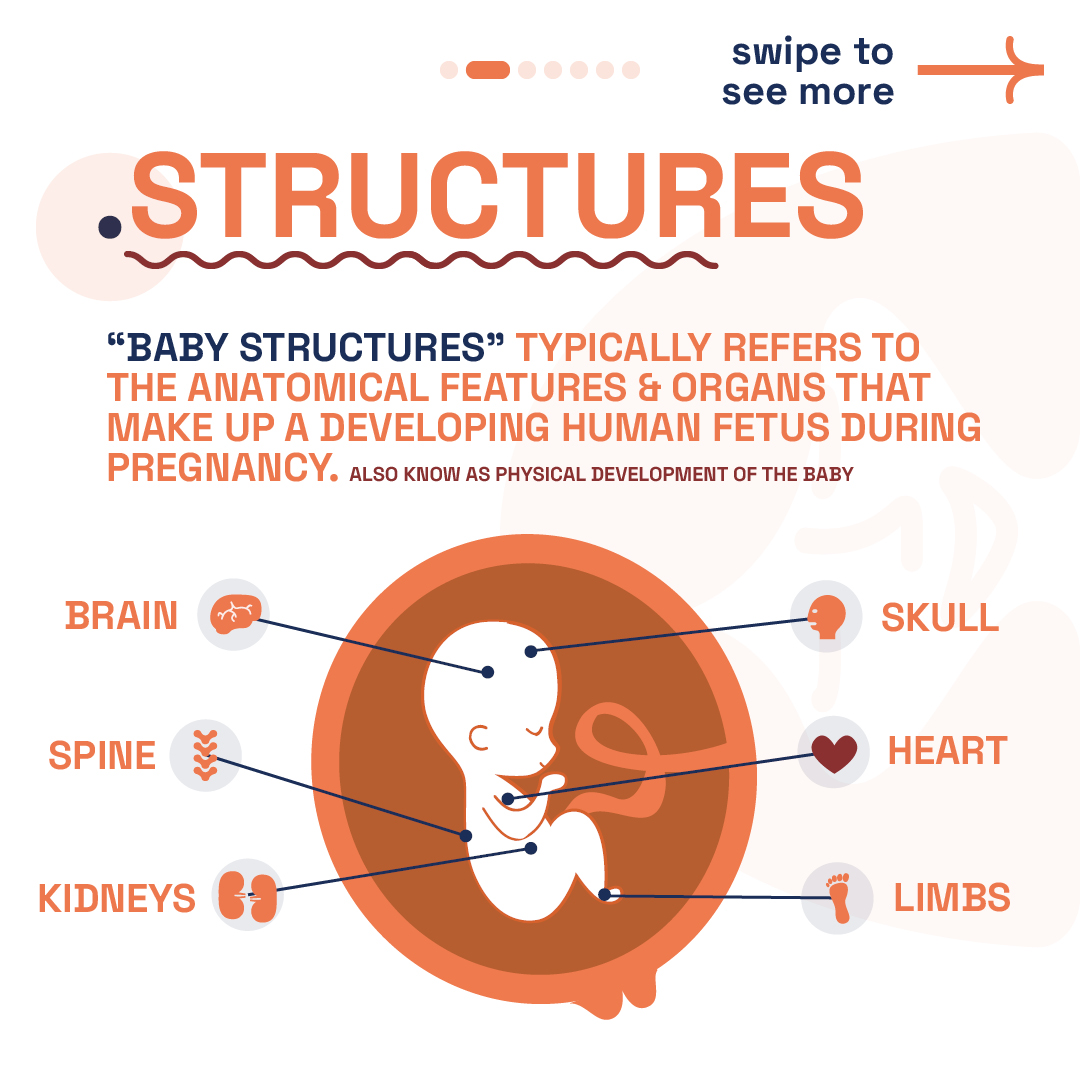
“Baby structures”, or fetal structures, usually denote the anatomical features and organs constituting a human fetus throughout pregnancy, also referred to as the physical development of the baby. It is important to note that this does not include genetic anomalies like Down Syndrome. Fetal development is a complex process where vital structures like the brain, heart, spine, and limbs evolve significantly:
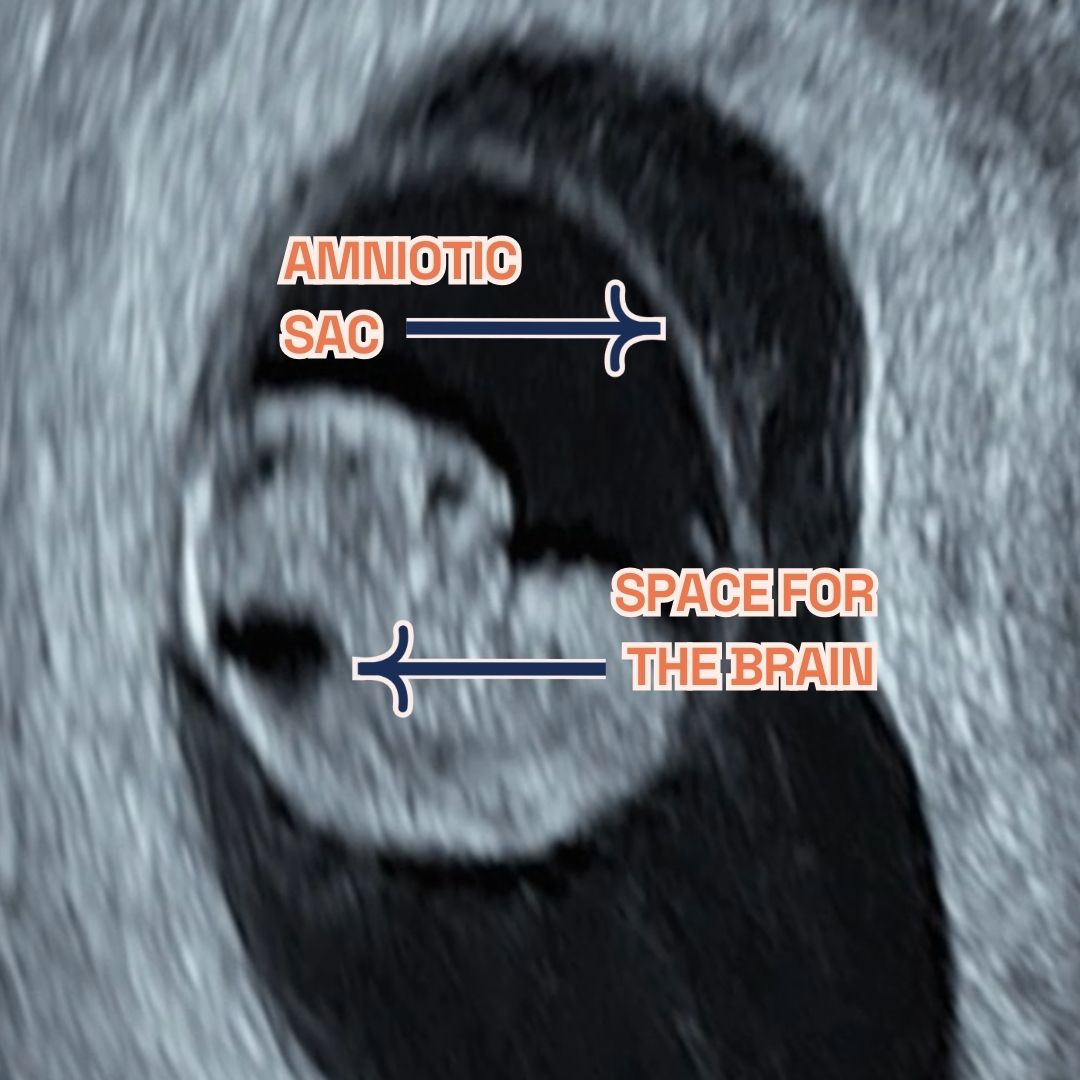
Brain: Development kicks off around week 5 with the neural tube, leading to the brain and spinal cord’s formation. By the second trimester’s close, the brain’s structure mirrors that of an adult, showcasing an almost fully developed brain stem.
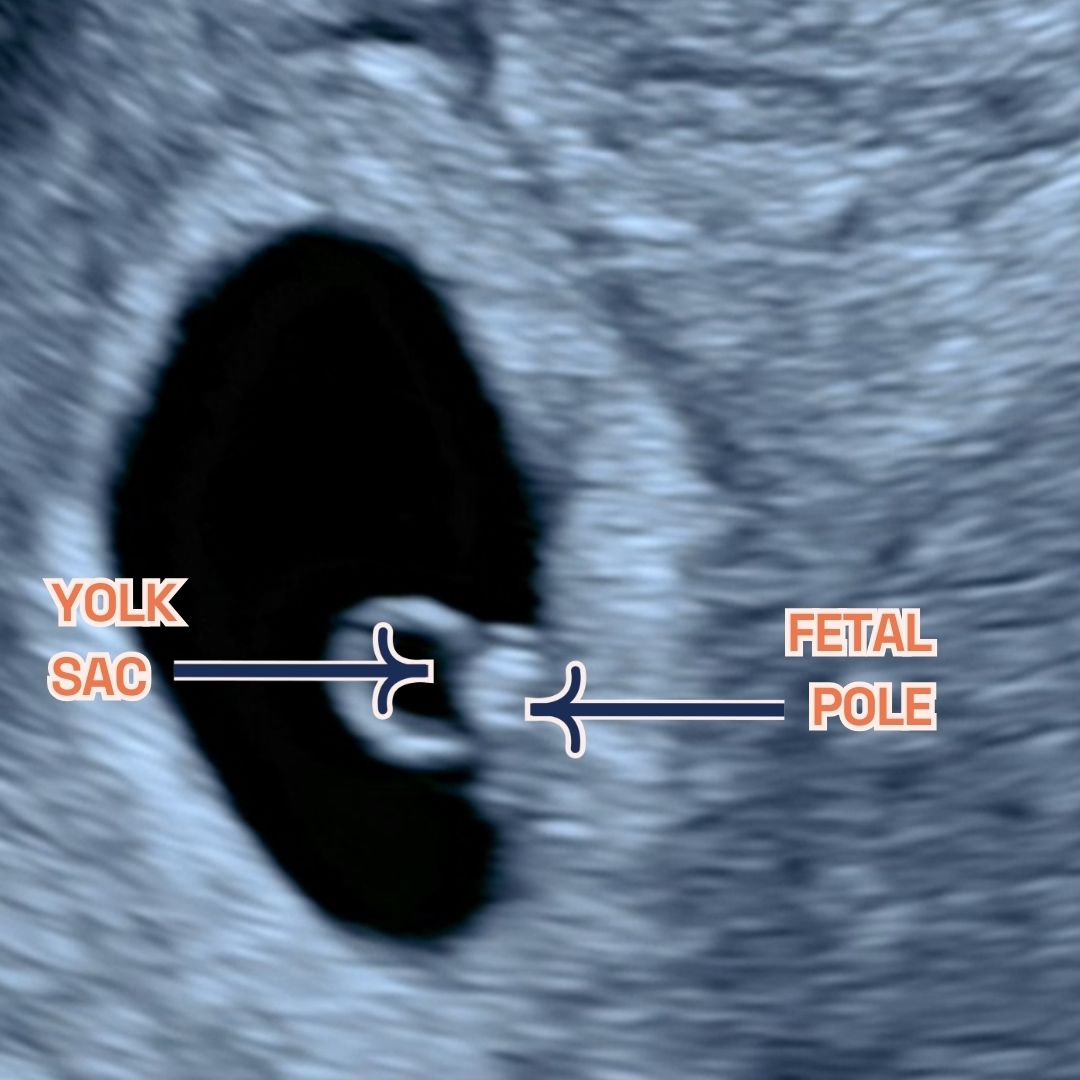
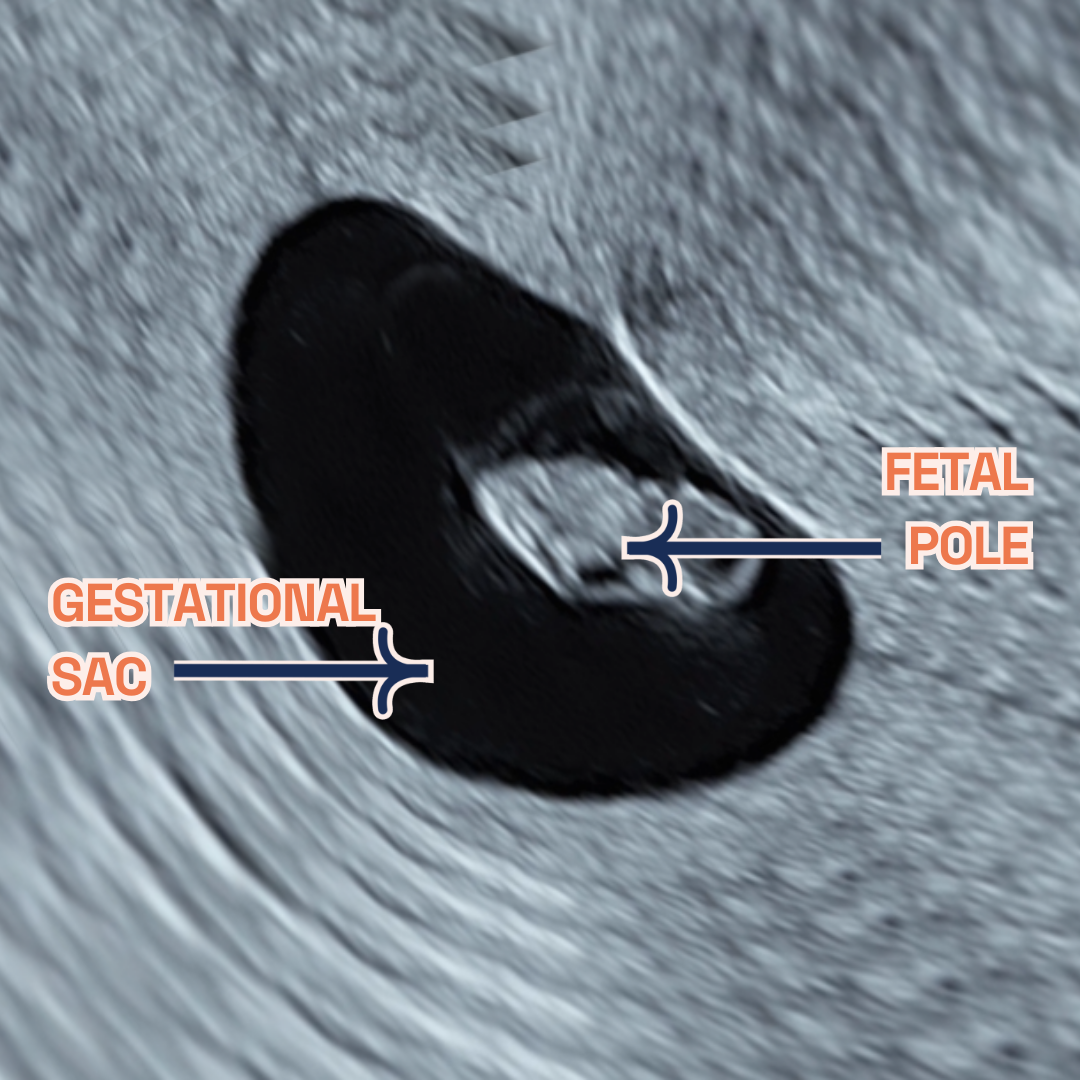
Heart: One of the earliest and most significant markers we observe during our dating scan is the heartbeat at 6 weeks, visible through ultrasound, providing crucial insight into the baby’s health and development at this early stage. This marks the beginning of the heart’s rhythmic life-sustaining beats.
Spine: The spine’s journey begins around weeks 6-7, laying the groundwork for the nervous system’s housing and body support. This period also sees the onset of bone development, integral to the body’s framework.
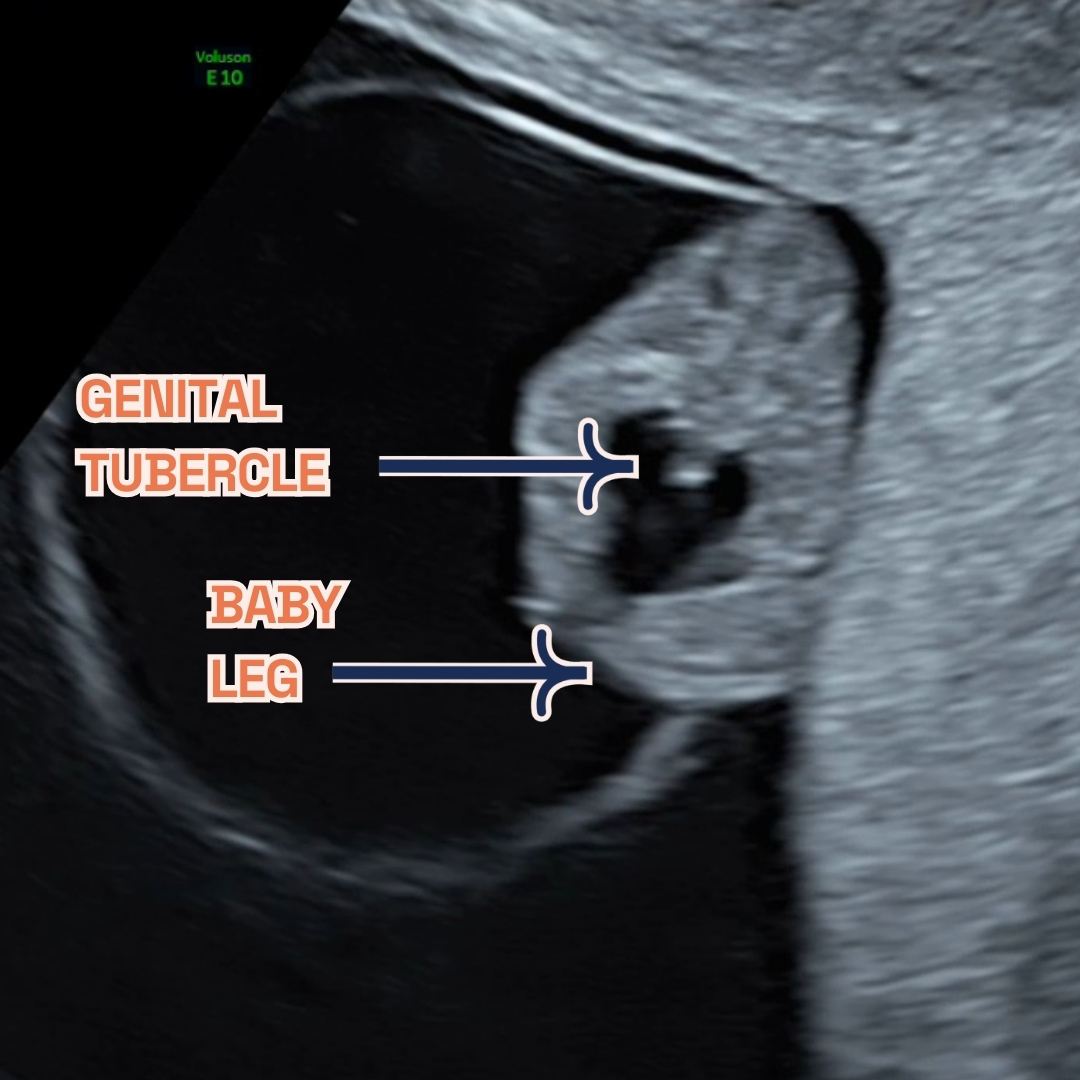
Limbs: Concurrently, weeks 6-7 see the emergence of arm and leg buds, with hands, feet, and digits evolving throughout the pregnancy. These developments are pivotal for the baby’s eventual movement capabilities.
The structures extend to encompass vital organs like the liver and kidneys, which are essential for processing nutrients and waste, the skull that protects the developing brain, and the umbilical cord, a lifeline connecting the baby to the placenta. Additionally, the abdominal organs, critical for digestion and other bodily functions, are part of this intricate network of development, underlining the complexity and wonder of fetal growth during pregnancy. Monitoring these structures’ growth is vital, employing fetal heart rate monitoring, ultrasounds, and physical exams to ensure the baby’s health and well-being.
Monitoring Key Baby Structures
Expectant mothers cherish every moment of their pregnancy journey, closely observing their baby’s development. The fetus’s organs and anatomical features, notably the brain, heart, spine, and limbs, undergo remarkable transformations. These critical structures not only signify health but also ensure the baby’s overall development and well-being.
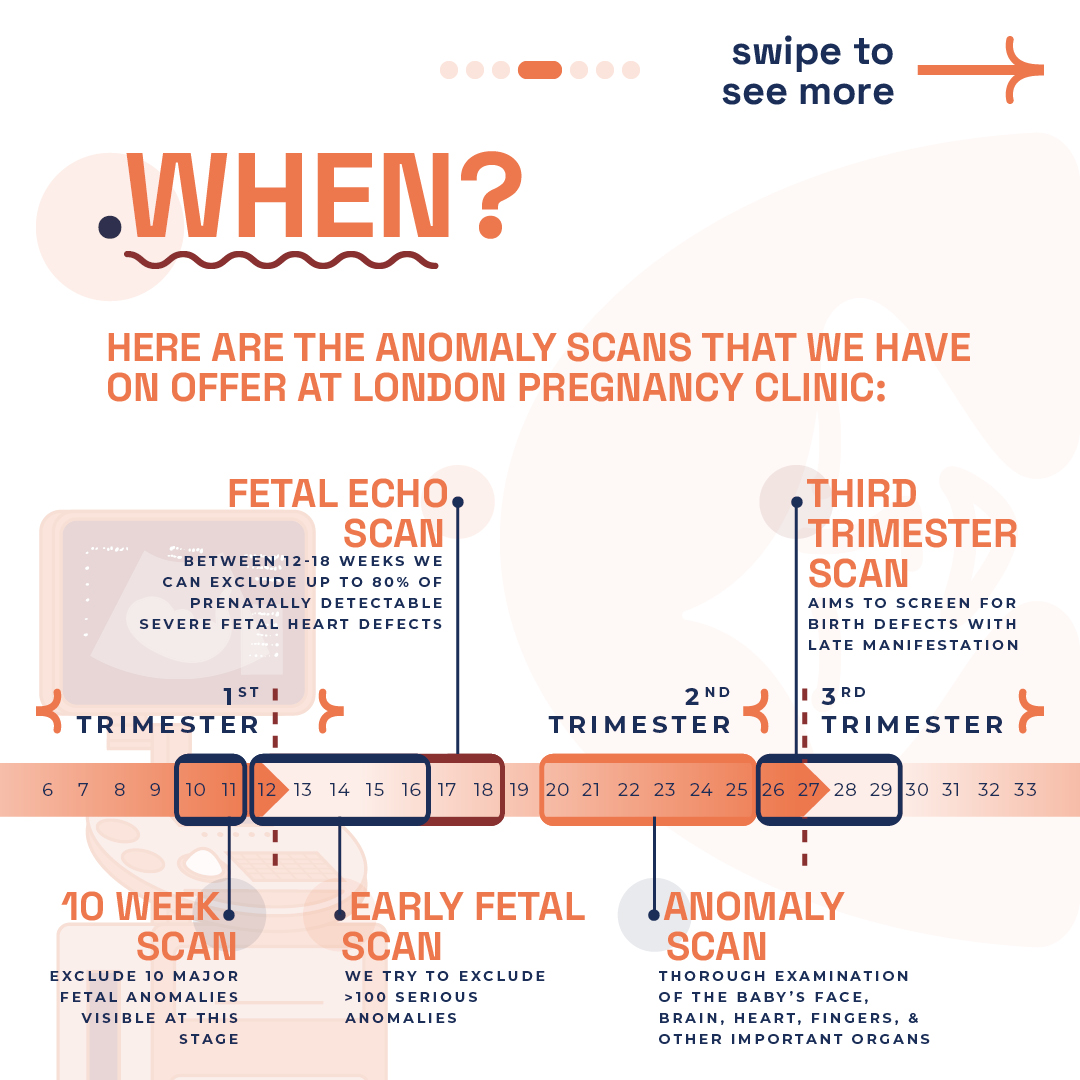
From the first to the third trimester, various scans are recommended to monitor your baby’s development. These range from the 10-week scan, aiming to exclude major fetal anomalies, to the fetal echo scan and the anomaly scan, each designed to screen for specific conditions at different stages of pregnancy .
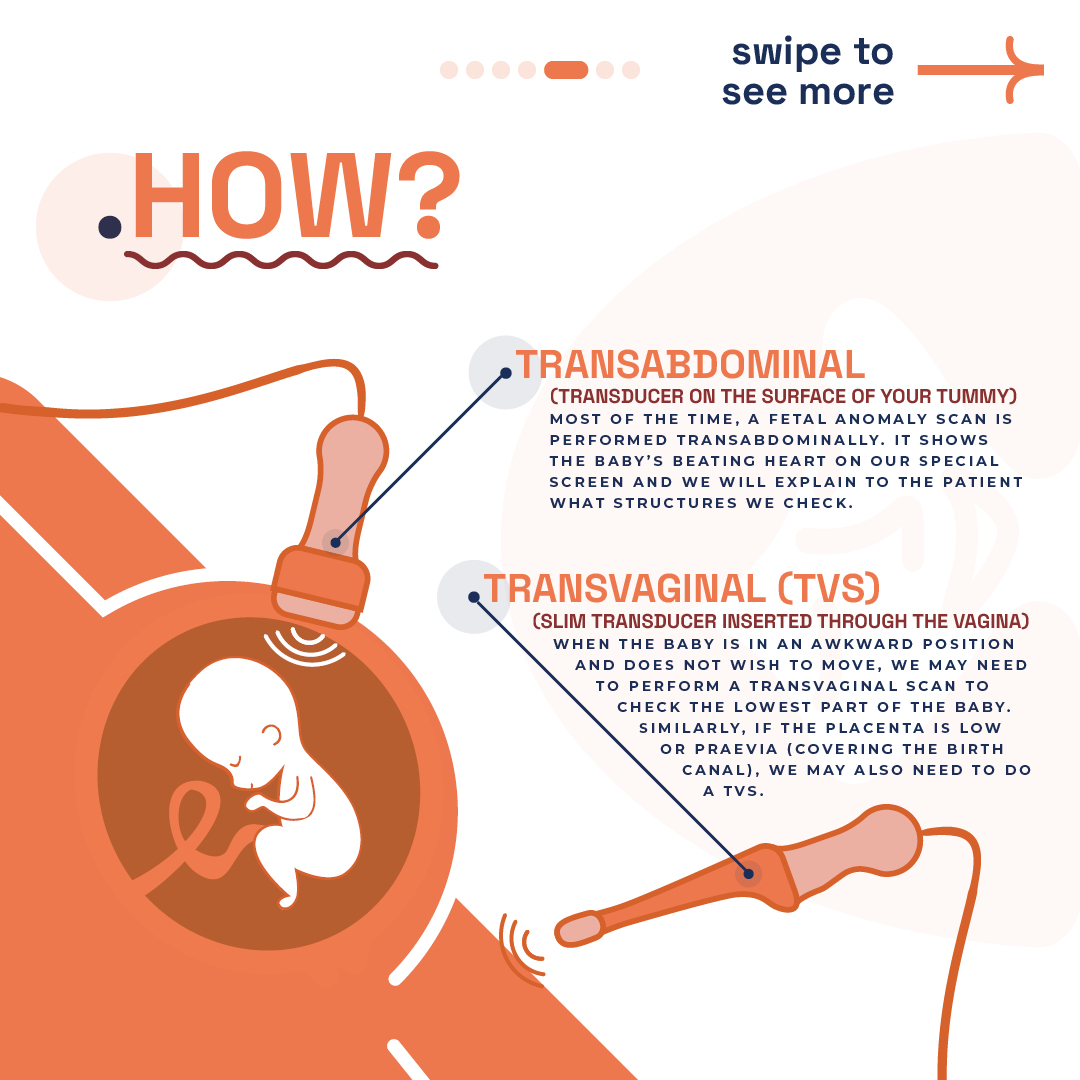
The majority of fetal anomaly scans are conducted transabdominally (watch our video on ultrasound probes), offering a glimpse of the baby’s heartbeat and structures. In certain cases, a transvaginal scan might be necessary for a more detailed view, especially when the baby is positioned awkwardly or when examining the placenta.
As the fetus grows, so does our anticipation and concern for its health. Regular monitoring of these structures becomes paramount. It reassures us that development proceeds without any hindrances. Specifically, we focus on the baby’s heart and brain, pivotal for life and cognitive functions. The spine’s integrity is equally crucial, supporting the body and housing the nervous system. Moreover, observing the limbs ensures proper growth and the potential for movement. In essence, these structures form the foundation of our baby’s future. Ensuring their optimal development through vigilant monitoring not only secures their health but also paves the way for a thriving life post-birth.
Most Common Structural Anomalies?
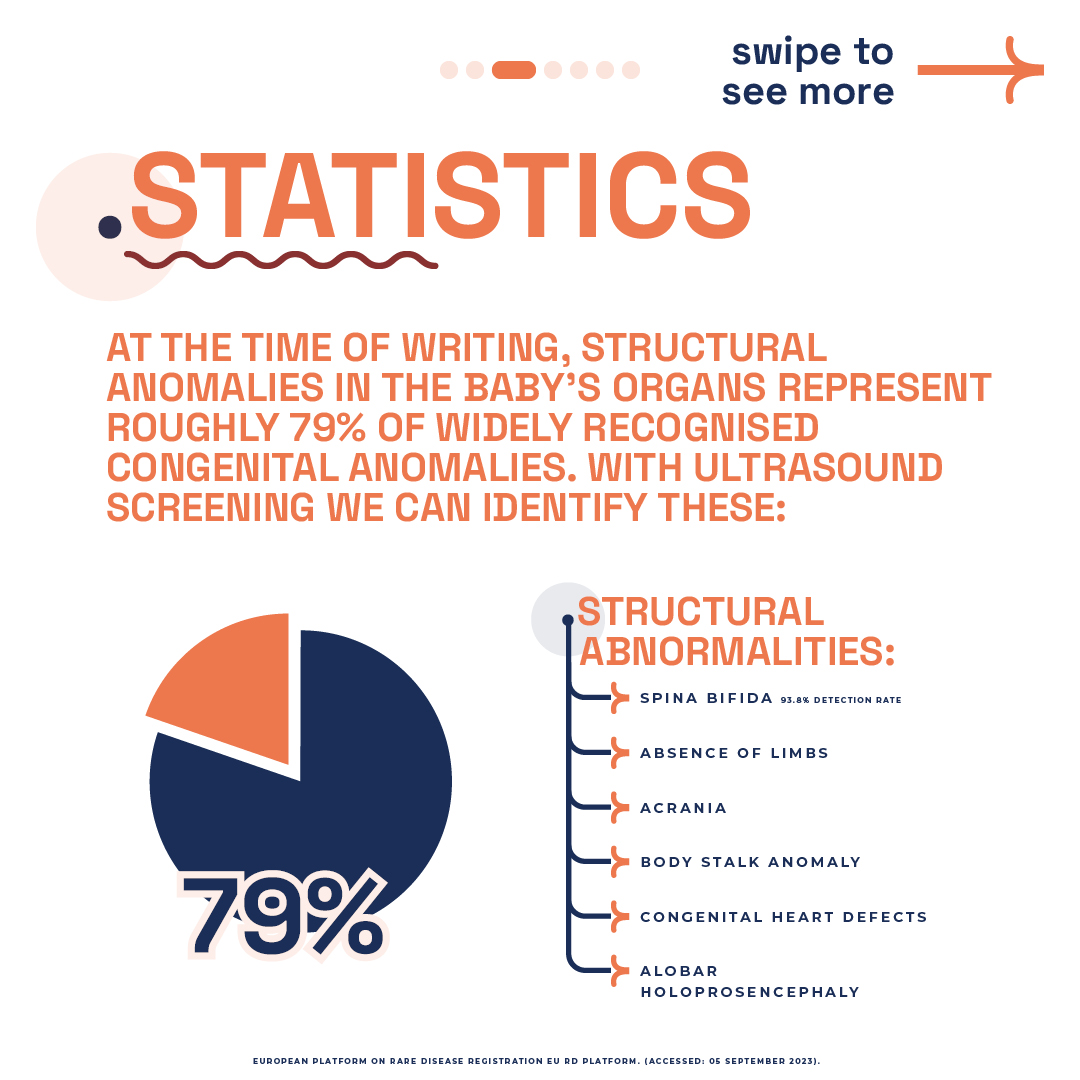
According to the European platform on Rare disease registration EU RD Platform, structural anomalies in the baby’s organs represent roughly 79% of widely recognised congenital anomalies. The most common structural anomaly encountered in newborns is congenital heart defects (CHD). These defects, which disrupt the heart’s structure and function post-birth, affect 1 in 100 UK babies. Ventricular septal defect (VSD), or ‘hole in the heart,’ stands out as the predominant issue.
Newborns also face other frequent congenital issues, including:
- Cleft Lip and Palate: A gap in the mouth’s upper lip and roof.
- Spina Bifida: The spinal column’s incomplete closure.
- Neural Tube Defects (NTD): Disorders like anencephaly affecting brain and spinal development. Spina bifida falls under NTDs.
- Gastroschisis: Intestines extending outside the abdomen from birth.
Exomphalos or Omphalocele: Abdominal organs bulge through the navel. - Clubfoot or Talipes: A foot deformity where it angles inwards and downwards.
- Limb Reduction Defects: Absence or incomplete limb formation.
- Polydactyly: Having extra fingers or toes.
- Intestinal and Duodenal Atresia: Intestine blockages or missing sections.
- Kidney Anomalies: Various kidney development, structure, or function malformations.
In essence, these conditions highlight the spectrum of potential challenges infants may face from birth, underscoring the importance of early detection and intervention. Awareness and understanding of these common anomalies can lead to better outcomes for affected children, as early intervention often opens the door to corrective procedures and supportive therapies, enhancing quality of life. The emphasis on these conditions reflects a commitment to providing the necessary care and support for affected families, guiding them through diagnosis, treatment, and beyond, with a focus on fostering resilience and hope.
Ultrasound Screening Vital for Early Detection
Ultrasound pregnancy scans transcend mere glimpses into the womb; they are indispensable tools in prenatal care. Structural anomalies within the baby’s organs account for a significant share of congenital anomalies. Fortunately, ultrasound offers a solution, detecting early signs of such conditions. At the London Pregnancy Clinic, our expertise in ultrasound screenings shines at every stage. We tailor our early pregnancy scans to the gestational age, offering unparalleled early detection from 10 weeks onwards.
10 Week Scan: Our clinic excels with a pioneering 10/11-week scan, designed to uncover 10 critical fetal anomalies early on. This scan, unique to our services, complements NIPT seamlessly, setting a new standard in prenatal care.
Early Fetal Scan: The hallmark of our service, the Early Fetal Scan, conducts an exhaustive review of the baby’s development. It’s crafted to spot over 100 serious anomalies well ahead of the standard NHS 19-20 week screenings. Offering this advanced insight provides early reassurance and essential information to expectant parents.
In short, our approach revolutionises prenatal screenings, giving you early answers and peace of mind. It brings to light potential issues, enabling timely interventions. These screenings are not just procedures but gateways to peace of mind for expectant mothers. They assure us that our baby’s development is on the right track, allowing us to address any concerns proactively.
-

Baby with missing left hand at 12 week, an absence or incomplete limb formation.
-

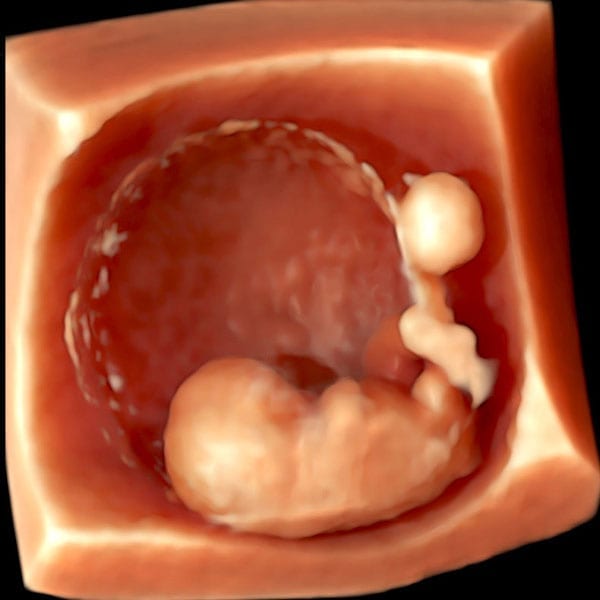
Normal baby at 12 weeks of pregnancy during an early pregnancy scans 3D.
Advanced Anomaly Detection in Late Pregnancy
Early detection of fetal anomalies enables timely interventions, crucial for the well-being of your baby. However, some anomalies manifest later, necessitating advanced screenings in the later stages of pregnancy. Our late-stage anomaly scans are designed to offer peace of mind and crucial insights during the final stages of pregnancy.
Anomaly Scan: Our 22-23 week Anomaly Scan goes beyond the NHS’s 19–20-week standard, offering a deeper insight into your baby’s development. This comprehensive check includes detailed assessments of the brain, heart, face, fingers, and vital organs. We also provide additional services like uterine artery Doppler and cervical length measurements on request, ensuring an all-encompassing review.
3rd Trimester Anomaly Scan: To address the absence of routine NHS scans post-18-20 weeks, our clinic offers the 3rd Trimester Anomaly Scan between 26-29 weeks. This scan is pivotal for detecting late-manifesting anomalies and monitoring fetal growth and well-being. Given the technical difficulties of scanning after 30 weeks, this period is optimal for identifying significant issues, especially affecting the brain, heart, and kidneys. It’s also an ideal time for clinical 3D/4D imaging, enriching your connection with your unborn child.
Leveraging state-of-the-art technology and thorough assessments, we are committed to delivering unparalleled prenatal care. Trust our expertise to navigate you through these essential phases of pregnancy, providing clarity, early intervention opportunities, and fostering a profound bond with your baby.
Why do we focus on Early detection?
At our clinic, early detection of fetal anomalies stands as a priority, underlining our commitment to comprehensive prenatal care. Early diagnosis paves the way for detailed insights into potential health issues, fostering a deeper understanding and effective management from the outset.
This early intervention allows healthcare experts to convey critical information regarding the anomaly, its possible effects, and the spectrum of care and intervention options available. Such a proactive stance equips parents with the knowledge to make well-informed decisions, streamlines medical planning, and guarantees the availability of essential support and resources.
Given the time-sensitive nature of advanced genetic screenings, including microarrays and exome sequencing, alongside expanded NIPT choices, securing an early diagnosis is crucial. These intricate tests, demanding several weeks for results, underscore the necessity of timely identification. It ensures ample time for exhaustive testing, facilitating a holistic and well-considered approach to prenatal care and support throughout the pregnancy journey.
Embracing this early detection strategy, we aim to guide expectant parents with clarity, empowering them with options and support every step of the way. Our focus on early diagnosis reflects our dedication to delivering exceptional care and support, ensuring a well-informed, reassuring pregnancy experience.
Baby Structures FAQs
-
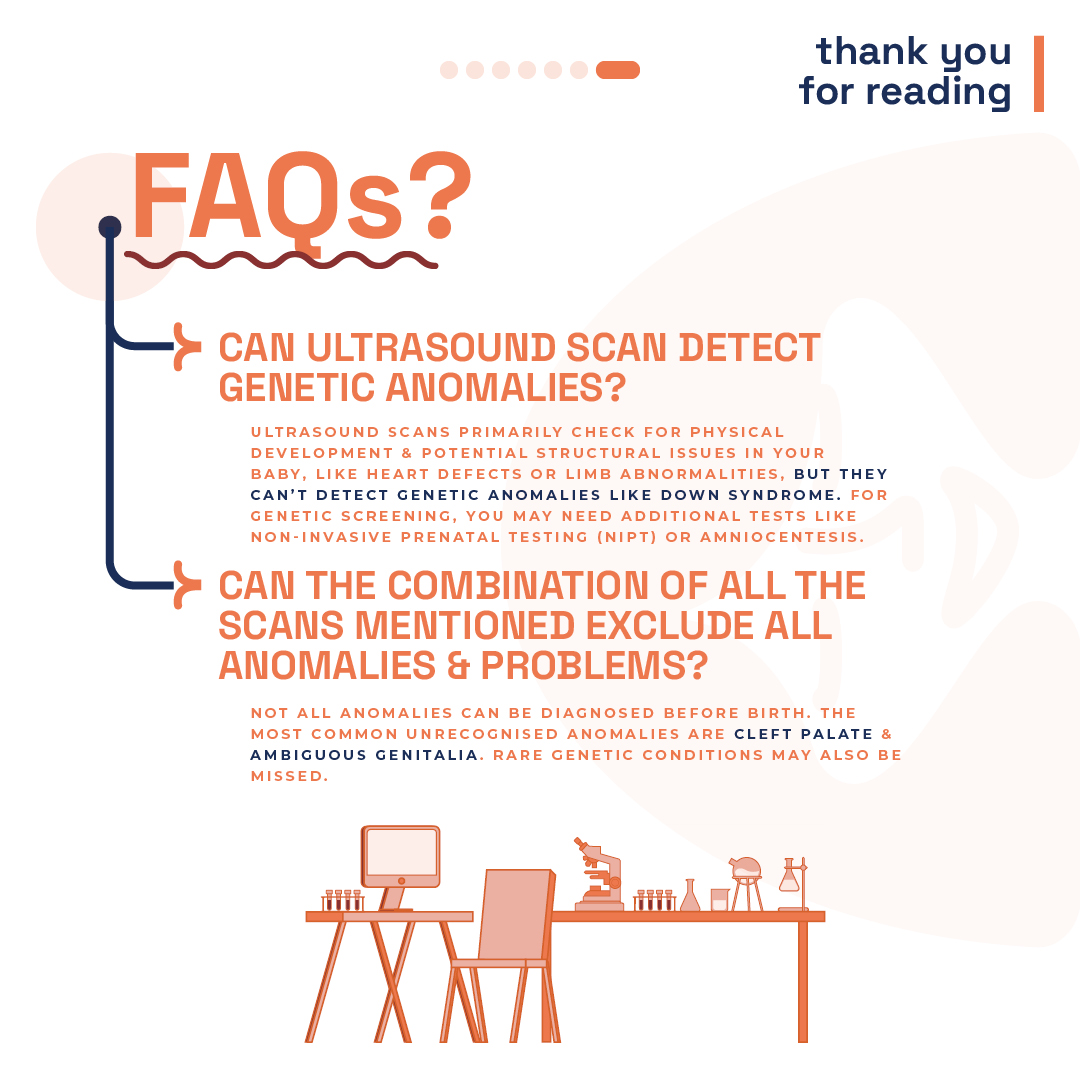
Can ultrasound detect genetic anomalies?
While ultrasound scans are adept at identifying physical development and potential structural issues, they cannot detect genetic anomalies. For genetic screening, additional tests like Non-Invasive Prenatal Testing (NIPT) or amniocentesis are recommended.
-
Do the scans guarantee the detection of all anomalies?
Regrettably, predicting every anomaly before birth is beyond reach. Commonly missed anomalies include isolated cleft palate (a split in the mouth’s roof with intact lips) and ambiguous genitalia. Additionally, certain rare genetic conditions elude detection through ultrasound scans.
-
Structural Anomalies Linked to Genetic Syndromes?
Noticing structural anomalies or physical differences in a baby during pregnancy often hints at a genetic or chromosomal connection. Simply put, these anomalies might signal an underlying chromosomal or genetic syndrome, commonly referred to as “rare diseases.”
Understanding the tie between genetic makeup and structural anomalies is key. It unravels the complex relationship between a baby’s DNA and their physical traits. An anomaly might stand alone or indicate a broader genetic condition.
If a baby is diagnosed with a chromosomal or genetic condition, these anomalies manifest the impact of irregular gene functions.
Crucially, when structural defects accompany chromosomal or genetic conditions, the prognosis tends to be more serious than isolated anomalies. Such conditions frequently correlate with intellectual disabilities or significant health issues, underscoring the importance of early detection and intervention.
-
Why do NIPT with Scan and visa versa?
Ultrasound plays a crucial role in fetal screening, essential for confirming viability and gestational age alongside NIPT submissions. While NIPT effectively screens for three chromosomal anomalies and other genetic conditions (specific to the panorama test), it doesn’t assess structural anomalies. Conditions like heart or brain defects, often more common and severe than Down’s syndrome, require ultrasound for detection.
At the London Pregnancy Clinic, our forte is the early identification of fetal anomalies, particularly in the fetal heart and brain. Remarkably, we’re capable of detecting significant anomalies from as early as 10 weeks. Discover more about the scans we pair with NIPT by visiting our scans page; our 10-week scan frequently stands out as the optimum choice.
Opting for a Panorama Test at 9 weeks? Rest assured, we’ll conduct a detailed structural scan of your baby, albeit with some limitations due to the embryo’s small size and early development stage.
Final Thoughts
Understanding the structures of your developing baby is a crucial part of the pregnancy journey. Ultrasound screenings offer an invaluable tool in this understanding, providing early detection of potential issues and contributing to the effective monitoring of your baby’s health. We invite you to experience the comprehensive care and advanced screening options available at the London Pregnancy Clinic, where we prioritise your peace of mind and your baby’s well-being.